Written by Jennifer Harris, MSc. 5/6/2024
Despite advances in medical treatment, people remain reluctant to get tested for infectious diseases, like HIV and HCV, due to fears of a positive test or related stigma and discrimination. For immigrants, who often do not have health insurance or a primary care physician, the fears and challenges are greater. Clinic-based HIV testing misses large swaths of the population who don’t regularly visit healthcare facilities1. One of the significant challenges for meeting the CDC’s goal of reducing new HIV infections by 90% by 2030 is to get a far greater number of people tested2. Similarly, the improvement in the number of people diagnosed with HCV infection is crucial to reach the World Health Organization’s objectives for eliminating viral hepatitis by 20303.Accessing people who are medically underserved is difficult for large governmental agencies, especially when a language barrier exists. Bringing point-of-care (POC) testing to a community instead is one approach that many find less stigmatizing.
What is the value of HIV and HCV co-screening? Full Video »
HBI's Mission
The Health Betterment Initiative (HBI) is a community-based organization specializing in building bridges to equitable healthcare for immigrants and other people who are medically underserved. HBI began almost 20 years ago as the Hepatitis B Initiative; primarily conducting liver health screens in the Asian immigrant community. HBI adopted a more comprehensive healthcare approach over time, expanding POC testing as an integral component of this larger model. The organization began free screening programs for HCV in 2013 and HIV in 2016.
Recently, OraSure Technologies, Inc. spoke with Sandra Marrero-Ashford, MPA, MPH, MA, executive director of HBI, about HBI’s journey in using rapid testing for underserved communities and linking people to requisite care.
"Our entry into providing care starts with testing," says Ashford, "but that's just the beginning. We educate people to eliminate stigmas along the way and know that impacting just one individual can lead to affecting a whole community."
Building Trust
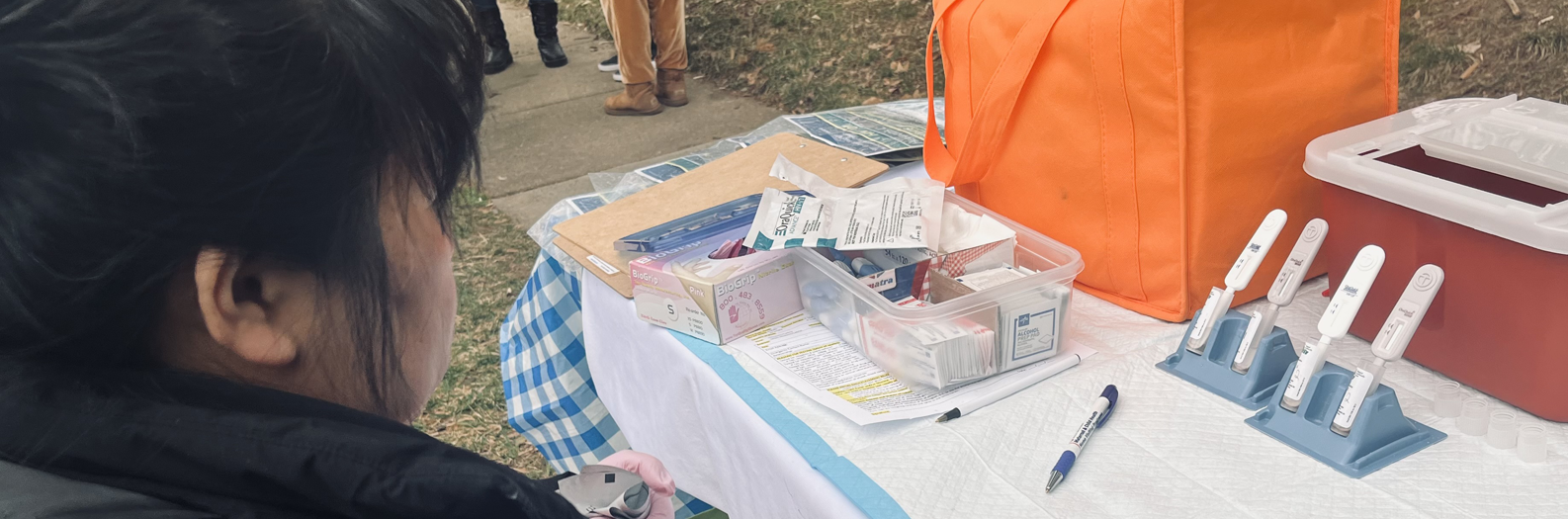
HBI tailors its outreach efforts to suit the unique demographics and locations of the communities it serves. Through collaborative partnerships, we provide culturally sensitive outreach and rapid testing services in various unconventional settings, including churches, homeless shelters, harm reduction organizations, substance abuse rehabilitation clinics, health fairs, senior centers, and small immigrant business centers. Additionally, our healthcare workers are skilled in languages such as Spanish, Mongolian, Chinese, Vietnamese, and Amharic, facilitating effective communication and trust-building.
Ashford highlights the impact of our HBI’s approach: "For example, our Mongolian community health worker has played a vital role in establishing connections within her community. Her fluency in their language has expanded our reach, as people trust her and are more willing to participate in testing."
"We integrate individuals with personal experience into our shelter testing program," Ashford elaborates. "These individuals have firsthand knowledge of addiction within their families or belong to LGBTQIA communities. This strategy fosters trust and eliminates barriers to accessing our services."
Capturing Coinfection - 1 Fingerstick 2 Results
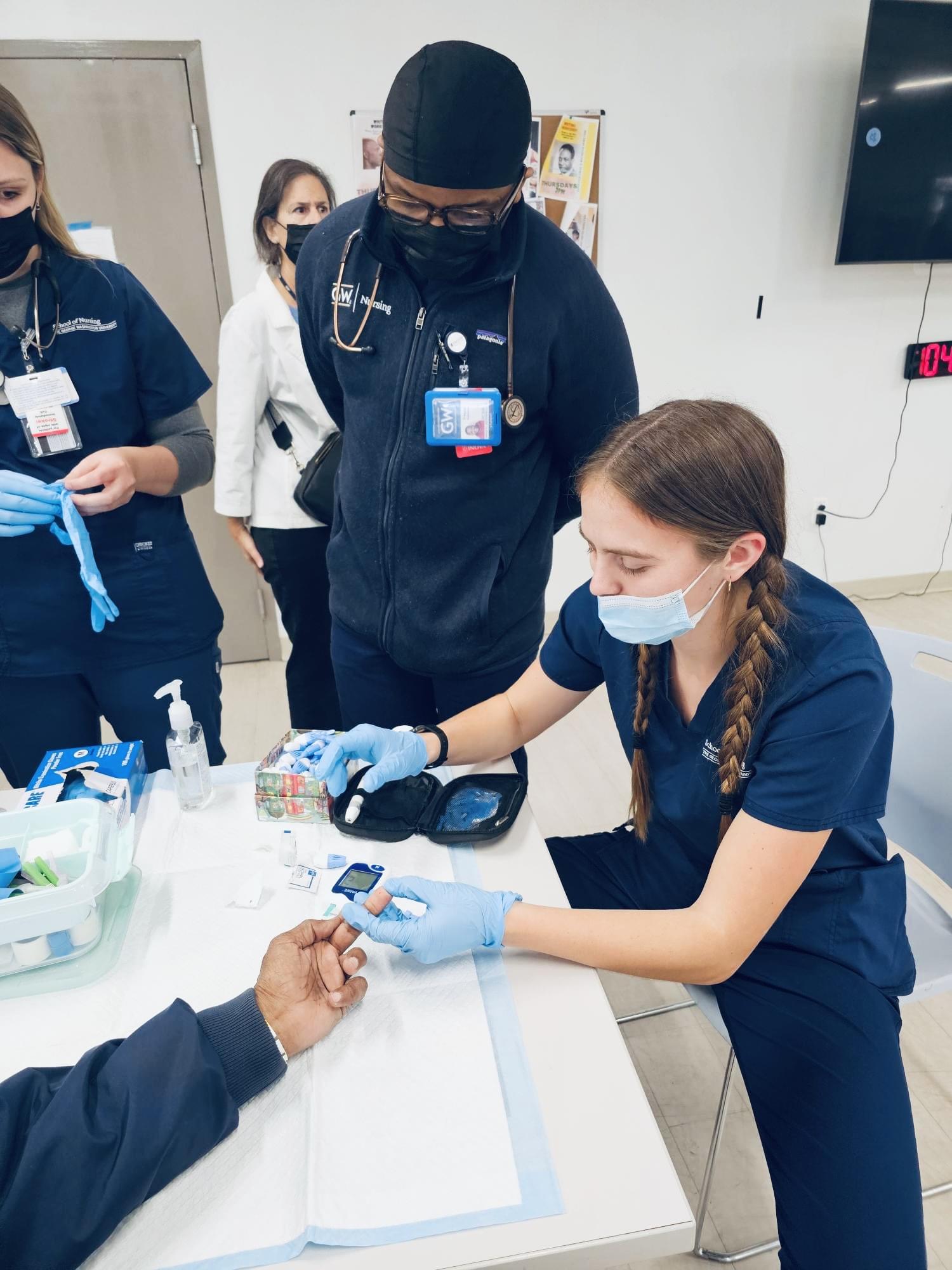
Health organizations are seeking innovative strategies, like community-based testing, to capture co-infections due to the fast increase of HIV and HCV cases. HBI uses OraQuick Advance® Rapid HIV-1/2 Antibody Tests and OraQuick® HCV Rapid Antibody Tests as part of their overall workflow. The tests can be run in parallel using a small blood sample from one fingerstick with results in 20 minutes. Participants learn their status for HIV and HCV in a single visit, which is critical for providing a continuum of care and stopping the spread of disease.
"Our healthcare workers can get both results from a single sample," says Ashford. "We can also do other health screenings, like glucose testing, and educate our clients in this time. If there’s a long line, we can start batch testing to make sure everyone is cared for."
Individuals co-infected with HIV and HCV may be at increased risk of transmitting both viruses to others. Hepatitis C is the most commonly reported bloodborne infection in the United States4. Odds of HCV infection were six times higher in people living with HIV (5·8, 95% CI 4·5–7·4) than their HIV-negative counterparts5. Effective testing services can help enable targeted prevention efforts and reduce the transmission of both viruses.
Early Detection
Early detection of co-infections allows for timely intervention strategies. These can include antiretroviral therapy for HIV and direct-acting antiviral medications for HCV, which are highly effective in controlling both infections when initiated early. Even people who test HIV negative can link to pre-exposure prophylaxis (PrEP), offering providers a care pathway to support on-going HIV prevention.
Rapid testing not only enhances accessibility but also mitigates the apprehension often associated with traditional testing methods. Moreover, our ability to swiftly connect clients to care is paramount, particularly for vulnerable populations such as people who inject drugs (PWID) and use drugs (PWUD), as well as the unsheltered individuals whom we HBI may only engage with for a brief period. In these instances, every moment is crucial in establishing sustainable care pathways for HIV and HCV.
"We were the perfect candidates to continue to test for hep C. The community already trusted us with hep B testing. The government actually approached us to expand our testing for HCV because we had built trust within the immigrant community," says Ashford. "It can be difficult to get people through the door when they don’t know you."
HBI has developed partnerships with health departments like the DC Health Department, Maryland Health Department and Virginia Health Department -- areas highly impacted by the HIV and HCV epidemics. These partnerships increase the footprint in a community and allow for a more efficient use of public health resources.
In the past few years, HBI has seen a lower percentage of HIV positive tests, but a higher percentage of reactive HCV and, in limited instances, syphilis test cases. Currently, HBI tests for syphilis only in the DC shelter area, but syphilis infections are also at epidemic levels requiring a targeted public health response. (OraSure is a licensed distributor for Diagnostics Direct Syphilis Health Check™ test.) HBI hopes to expand syphilis testing services in the future.
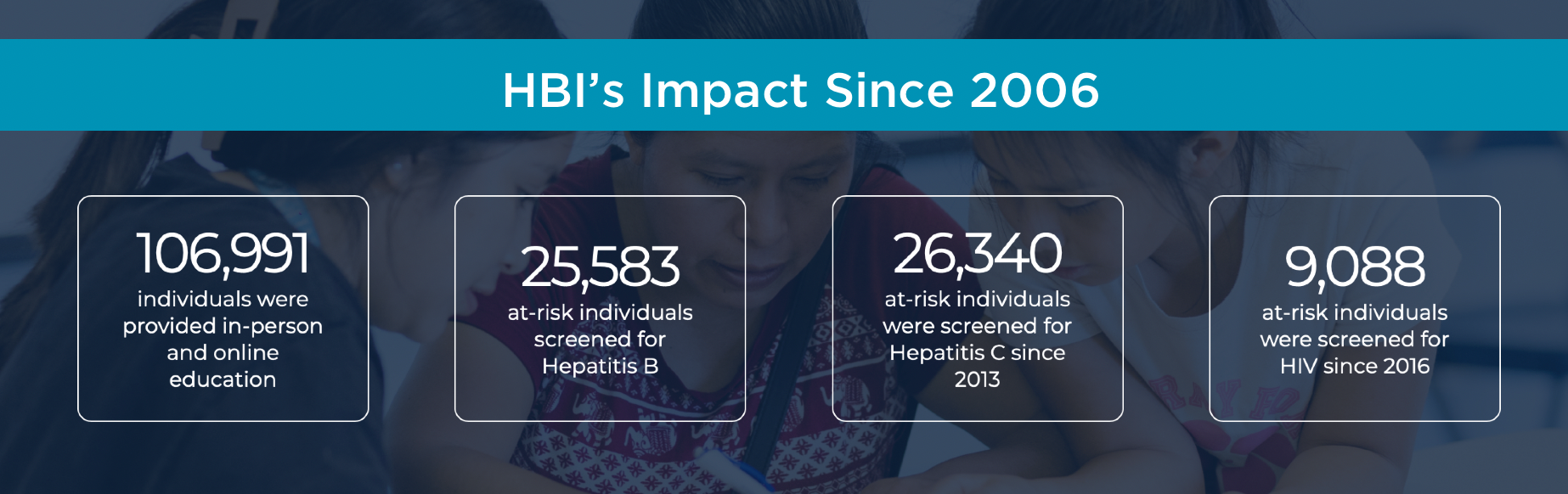
Overall, research has found community-based testing to increase uptake, identify new cases, be cost-effective, and effectively link many patients to care. Since 2013, HBI has screened 26,340 individuals for HCV, and 9,088 individuals for HIV as of 2016. Countless other participants of HBI’s outreach programs have been linked with educational and health resources in their communities.
OraSure is proud to offer diagnostic devices that support the research and wellbeing of sexual health. For more information regarding OraSure's entire infectious disease portfolio, please view our
OraSure is proud to offer diagnostic devices that support the research and wellbeing of sexual health. For more information regarding OraSure's entire infectious disease portfolio, please view our Rapid Infectious Disease Products . If you are interested in case studies, webinars and other industry perspective, please visit IDX Insights.
References:
1 Levy, M.E., Wilton, L., Phillips, G. et al. Understanding Structural Barriers to Accessing HIV Testing and Prevention Services Among Black Men Who Have Sex with Men (BMSM) in the United States. AIDS Behav 18, 972–996 (2014).: https://doi.org/10.1007/s10461-014-0719-x)
2 Nosyk B, Fojo AT, Kasaie P, Enns B, Trigg L, Piske M, Hutchinson AB, DiNenno EA, Zang X, Del Rio C. The Testing Imperative: Why the US Ending the Human Immunodeficiency Virus (HIV) Epidemic Program Needs to Renew Efforts to Expand HIV Testing in Clinical and Community-Based Settings. Clin Infect Dis. 2023 Jun 16;76(12):2206-2208. doi: 10.1093/cid/ciad103. PMID: 36815334; PMCID: PMC10273343.
3 Feld JJ, Ward JW. Key Elements on the Pathway to HCV Elimination: Lessons Learned From the AASLD HCV Special Interest Group 2020. Hepatol Commun. 2021 May 3;5(6):911-922. doi: 10.1002/hep4.1731. PMID: 34141979; PMCID: PMC8183173.
4 Hepatitis. https://www.who.int/health-topics/hepatitis/elimination-of-hepatitis-by-2030
5 Platt, Lucy, et al. "Prevalence and burden of HCV co-infection in people living with HIV: a global systematic review and meta-analysis." The Lancet infectious diseases 16.7 (2016): 797-808.
OraQuick is a registered trademark of OraSure Technologies, Inc. Syphilis Health Check is a trademark of Diagnostics Direct, LLC, used under license by OraSure Technologies, Inc.
